






When billing for ophthalmic diagnostic tests, consider several factors. Chart notes should support indications, orders and interpretations. Billers and coders must adhere to the various rules and payment restrictions.
In this article, we’ve summarized the pertinent information that applies to tests performed in a retina service.
Indications
Medical necessity for services should be clearly documented in the medical record. For coverage, diagnoses recorded in charts and on claims must be on the approved indications lists in payer policies and coverage articles. Policies are updated often, so check the payers’ websites frequently. Coincidentally, Palmetto GBA has published future policies that will be in effect in 2025 for both scanning computerized diagnostic imaging (codes 92133, 92134) and angiogram (codes 92235 – 92242).
Orders
Diagnostic tests not personally performed by the physician (for example, gonioscopy and extended ophthalmoscopy) require a documented physician’s order. This is usually noted as part of the plan in the record. Notes such as “VF today”, “OCT retina next visit.”
Payers expect the physician ordering the test will use the test in treating the patient.1 Medicare’s regulation states “Tests not ordered by the physician who is treating the beneficiary are not reasonable and necessary.” This means that he or she is managing the disease for which the test was ordered. Standing orders are not acceptable.
Usually, the order is preceded by a physician’s examination of the patient that determined the need for the test. In rare cases, a physician may place the order prior to an exam based on specific information about the patient’s unique illness, injury or medical condition provided by another physician, or perhaps the patient. Examples include:
- An ophthalmologist reviews the chart notes from a referring doctor and orders a diagnostic test to be administered upon the patient’s arrival.
- A technician notes something concerning when taking a history from a new patient. The technician shares this information with the physician and an order for an immediate diagnostic test is made, based on it.
- An established patient calls and speaks to the physician, who orders a diagnostic test based on the phone call.
Supervision
CMS2 issues instructions specifying that diagnostic tests must “… be performed under the supervision of an individual meeting the definition of a ‘physician’ to be considered reasonable and necessary and, therefore, covered under Medicare.”3
Medicare has established three different levels of physician supervision, commensurate with the risk to the patient and/or the skills required to obtain useful results:
- General supervision, which means the procedure is furnished under the physician’s overall direction and control, but the physician’s presence is not required during the performance of the procedure.
- Direct supervision in the office setting, which means the physician must be present in the office suite and immediately available to furnish assistance and direction throughout the performance of the procedure.
- Personal supervision, which means a physician must be in attendance in the room during the performance of the procedure.
For various reasons, some tests do not have a supervision level assigned. Some are personally performed by the physician (eg, 92020, 92100). Some were added to CPT yet CMS never got around to assigning a supervision level (eg, 92025, 92136). Some are performed very infrequently (eg, 92260, 92287). Category III codes do not have a defined technical component (-TC) or professional component (-26), so supervision levels do not apply.
Interpretation
For many diagnostic tests, CPT’s description includes the phrase “with interpretation and report.”4 Documentation of the interpretation is important. Insufficient notes could lead to recoupment of payment.
The Medicare Claims Process Manual (MCPM) Chapter 13 §100, Interpretation of Diagnostic Tests5 makes a distinction between a review of a test and an “interpretation and report.”
“Carriers generally distinguish between an ‘interpretation and report’ … A professional component billing based on a review of the findings of these procedures, without a complete, written report similar to that which would be prepared by a specialist in the field, does not meet the conditions for separate payment of the service. This is because the review is already included in the … E/M payment.”
An interpretation is described as:
An ‘interpretation and report’ should address the findings, relevant clinical issues, and comparative data (when available).”
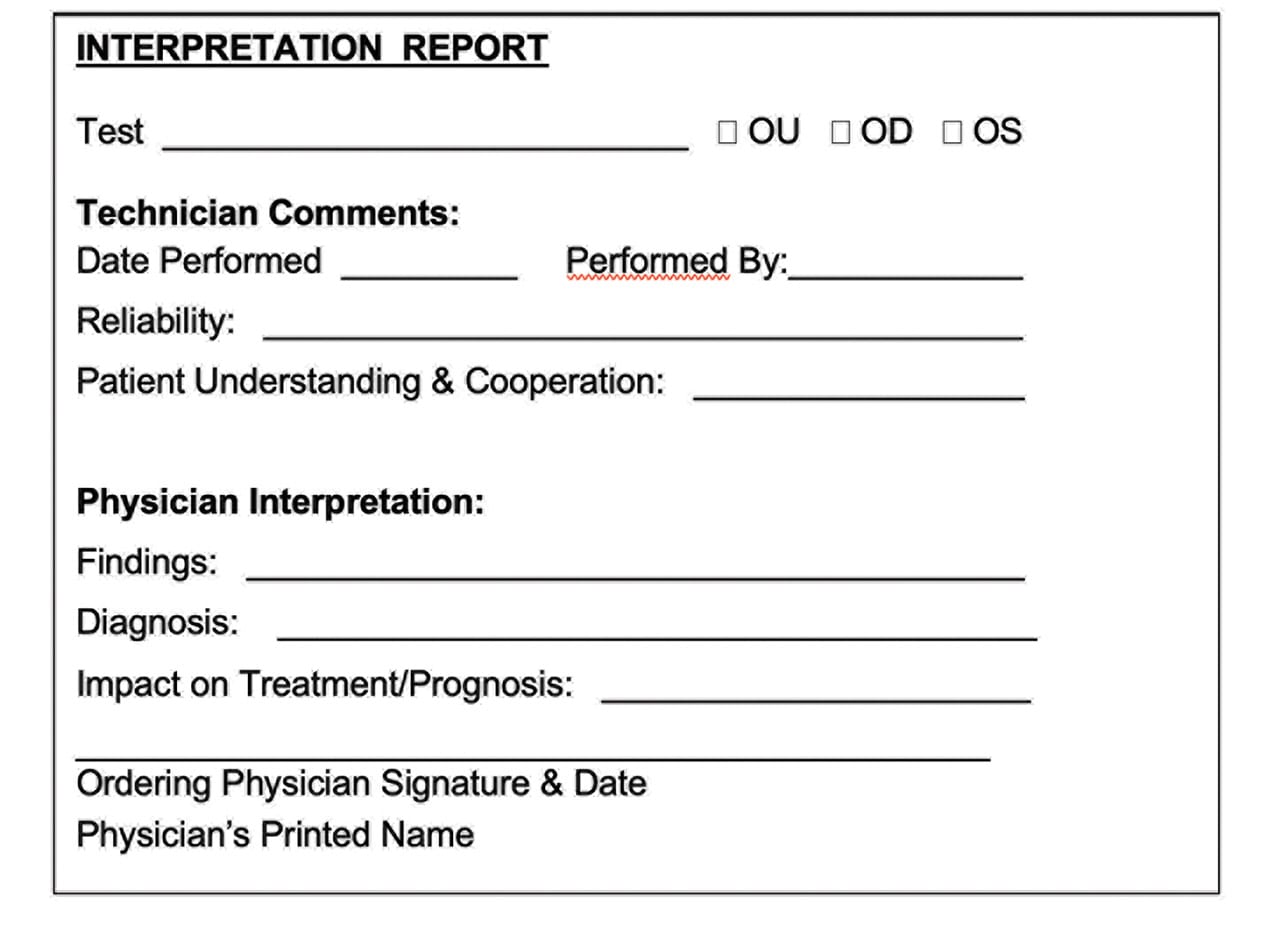
Simple, brief notations such as “normal” or “abnormal” constitute a review of the test rather than an interpretation and report. The interpretation and report must answer pertinent questions about the service.
- Physician’s order – Why is the test desired?
- Date performed – When was it performed?
- Technician’s initials – Who did it?
- Reliability of the test – Was the test of any value?
- Patient cooperation – Was the patient at fault?
- Test findings – What are the results of the test?
- Assessment, diagnosis – What do the results mean?
- Impact on treatment, prognosis – What’s next?
- Physician’s signature – Who is the physician?
Some tests — such as perimetry — provide more valuable information when there is a series. Then, the “comparative data” mentioned above is particularly meaningful. Adding a comment regarding stability or progression of the condition is helpful.
Within electronic records, the physician’s interpretation is often in a designated forced entry field. If the interpretation is written as part of the office visit note, it might appear to be an element of the exam and therefore missed by a reviewer. Try to differentiate it from the rest of the eye exam by surrounding the notations. Consider a format that could be used for diagnostic tests.
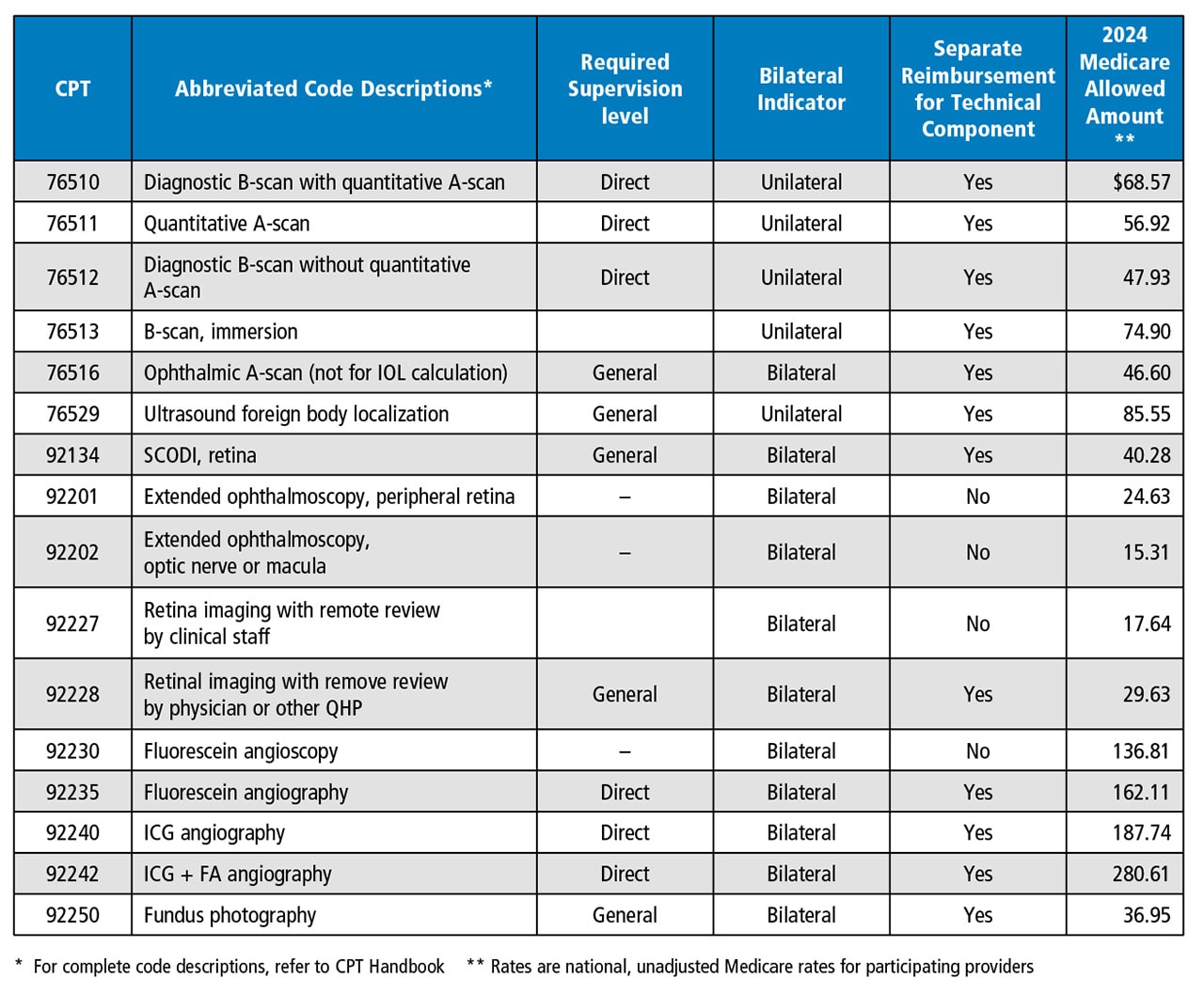
In the Medicare Physician Fee Schedule, different payment rates are established for the professional and technical components of a diagnostic test. Modifiers 26 and TC are used to identify the professional and technical portions. When TC and 26 are not appended to a CPT code, then the payer understands that reimbursement is sought for both the technical and professional components together in a single payment.
Unilateral vs Bilateral
CPT code descriptions do not usually specify “unilateral or bilateral,” but the Medicare Physician Fee Schedule does. Some ophthalmic diagnostic tests are unilateral (paid per eye), and others are paid the same whether one or both eyes are tested.6 Other third-party payers frequently follow Medicare’s indicators but are not obligated to do so and may establish their own rules.
Repeat Testing
Repeated testing is necessitated by the status of the disease and its, the advent of new disease, or planning for additional surgical treatment.
Screening Tests
As a general rule, tests performed as baseline documentation of a healthy eye, or to screen for potential disease, are not covered by Medicare and many medical insurance plans.
For screening tests, collect your fee from the patient. Use an appropriate financial waiver notice prior to providing the service.
Prohibited Code Combinations
CMS instructs the Medicare contractors to treat some concurrent procedures as a “bundle” or “mutually exclusive” for payment purposes. This means that no separate payment is made for the bundled service. The National Correct Coding Initiative is the regulation that updates these payment rules quarterly. Some other third-party payers have local policies with additional limitations.
Conclusion
Ophthalmologists have an assortment of diagnostic tests in their arsenal. Generally, each test requires an order and an interpretation. The remaining issues of billing and coding vary depending upon the test.
This discussion is meant to assist the reader to better understand the rules and regulations regarding reimbursement for often performed retinal diagnostic tests; however, appropriate usage, adequate documentation and proper coding are always the physician’s responsibility. OP
References:
1. Code of Federal Regulations, 42 CFR §410.32. Medicare Fee for Service Payment. https://www.ecfr.gov/current/title-42/chapter-IV/subchapter-B/part-410/subpart-B/section-410.32. Accessed Dec. 23, 2021.
2. As of June 14, 2001, the federal agency known as the Health Care Financing Administration (HCFA) became the Centers for Medicare & Medicaid Services (CMS).
3. HCFA Program Memorandum, Transmittal B-01-28, April 19, 2001. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/B0128.pdf. Accessed Dec. 23, 2021.
4. The Medicare Physician Fee Schedule multiple procedure indicator identifies these codes each year (multiple procedure indicator 7).
5. CMS. Medicare Claims Processing Manual (MCPM) Chapter 13 §100. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c13.pdf. Accessed Dec. 23, 2021.
6. Bilateral and unilateral services are identified in the Medicare Physician Fee Schedule each year.
