







Cataract surgery is the most common outpatient procedure performed in this country. As such, it is imperative that ophthalmic technicians understand the role they play in surgical outcomes. They are often the personnel acquiring the scans and data the surgeon will use to determine implant options with the patient. As technicians, we work alongside the surgeon to provide valuable and reliable diagnostic information.
Surgeons have a wide variety of diagnostic equipment to utilize when choosing implant types and powers that will work best for their patients. In this article, we focus on the most common diagnostic tests ordered and share tips technicians can use for acquiring accurate results.
FIRST, A PRIMER ON BIOMETRY AND KERATOMETRY
To start, we need to discuss biometry and keratometry readings. For the purpose of this article, we will discuss refractive errors in terms of axial length (how long the globe is) and keratometry (the shape of the cornea); we are excluding lenticular astigmatism and other pathology.
Axial length readings are typically acquired via ultrasound biometry (think A-scans) or laser optical biometers (think Lenstar [Haag-Streit], ARGOS [Alcon], IOLMaster [Zeiss]). Keratometry readings are determined by using corneal topographers, manual keratometers, or the topography readings often included in laser optical biometers. As a diagnostic technician, you may find that your surgeon utilizes multiple methods of keratometry for a single patient.
Typically, when selecting an intraocular lens (IOL), the surgeon will determine which set of keratometry readings he or she prefers. For example, during a cataract evaluation the surgeon orders a laser optical biometer, manual keratometry, and a corneal topography. The surgeon will then evaluate those measurements alongside the axial length and determine which set of keratometry readings he or she wishes to choose.
If the keratometry readings chosen are from the optical laser biometry, then no further keratometry adjustments are required in the biometer. If the surgeon selects keratometry readings from the manual keratometer or the corneal topographer, the technician will need to go back into the biometer and manually input the chosen keratometry readings. You will notice that this may change the IOL powers and refractive error projections.
In general terms, the power of the IOL is determined by the refractive power of the eye. Depending on the biometer used, the surgeon can gather valuable data in selecting the correct IOL power. When using a laser optical biometer, the measurements you gather are then calculated using a variety of formulas. After the formulas are complete, a page is then generated with IOL powers and projected refractive outcomes alongside other measurement data and reliability. A common formula you might see is the Barrett formula. Depending on the axial length, you may need to select a different formula to generate the IOL calculation page.
RELIABILITY IS CRUCIAL
A vital component for correct calculation of these algorithms is the reliability of the measurements taken. When performing biometry or keratometry, you must be careful to retake any measurements that appear unreliable. We’ll discuss what makes measurements unreliable in more detail below.
As technicians, we are highly valuable when we take on the task of troubleshooting for our doctors. Precious clinical time is wasted when a patient has waited for the doctor, only for the provider to realize that one or more of the scans need repeating.
GET A COMPLETE PICTURE
It is very common to have different technicians perform the in-room workup and the testing. As a technician in the testing role, you can put yourself at a disadvantage by neglecting to review your patient’s exam prior to proceeding with measurements. While looking through the patient’s workup, it is important to note the patient’s best-corrected visual acuity and refractive error.
Both values help to paint a picture of the patient’s current functionality. Not only will this aid in guiding the patient through areas of the clinic, but a wise technician will also use this information to predict the reliability of their measurements.
Consider, first, the biometry surgeons use to evaluate axial length. Refractive error often correlates with axial length. A normal axial length is around 24 mm. Patients who are hyperopic have a shorter axial length, while those who are myopic have a longer axial length. A testing technician with a strong background anticipates the axial length values and repeats any outlier measurements.
HOW TO AVOID UNRELIABILITY
Be warned that there is plenty of room for error when performing laser optical biometry regarding patient fixation. Optical biometers provide a fixation target and rely heavily on steady fixation. An asymmetric best-corrected visual acuity, when one eye can read multiple lines lower than the other, can suggest pathology that impacts an eye’s ability to maintain fixation, such as dense cataracts or amblyopia.
When noting an asymmetric acuity, it is wise to patch the stronger fellow eye while measuring the patient’s poorer seeing eye, allowing the opportunity for the weaker eye to find the target light.
Observing decentered corneal light reflexes during optical biometry can also hint at poor fixation. In a patient with strabismus, patching the fellow eye for each scan will increase the doctor’s confidence in the testing.
An ultrasound biometer can be more reliable when the patient struggles to fixate, as it does not require steady patient fixation nearly as much as a laser optical biometer. Ultrasound will measure axial length through dense cataracts better than an optical biometer. Ultrasound does, however, require more advanced skills as the probe or encompassing shell will sit on the globe. Keep in mind that too much pressure on the cornea can falsely shorten the captured axial length.
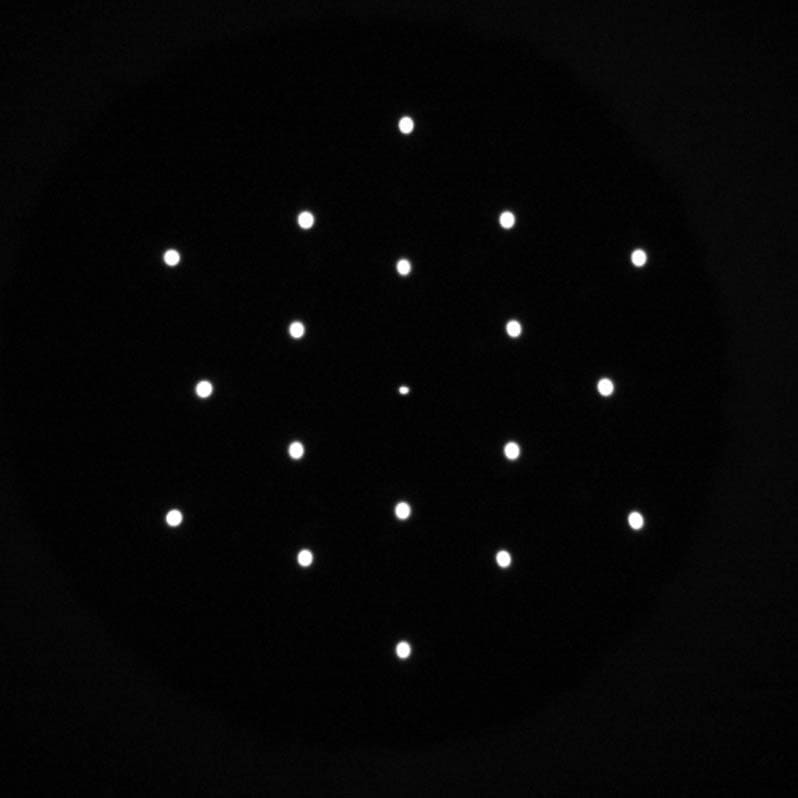
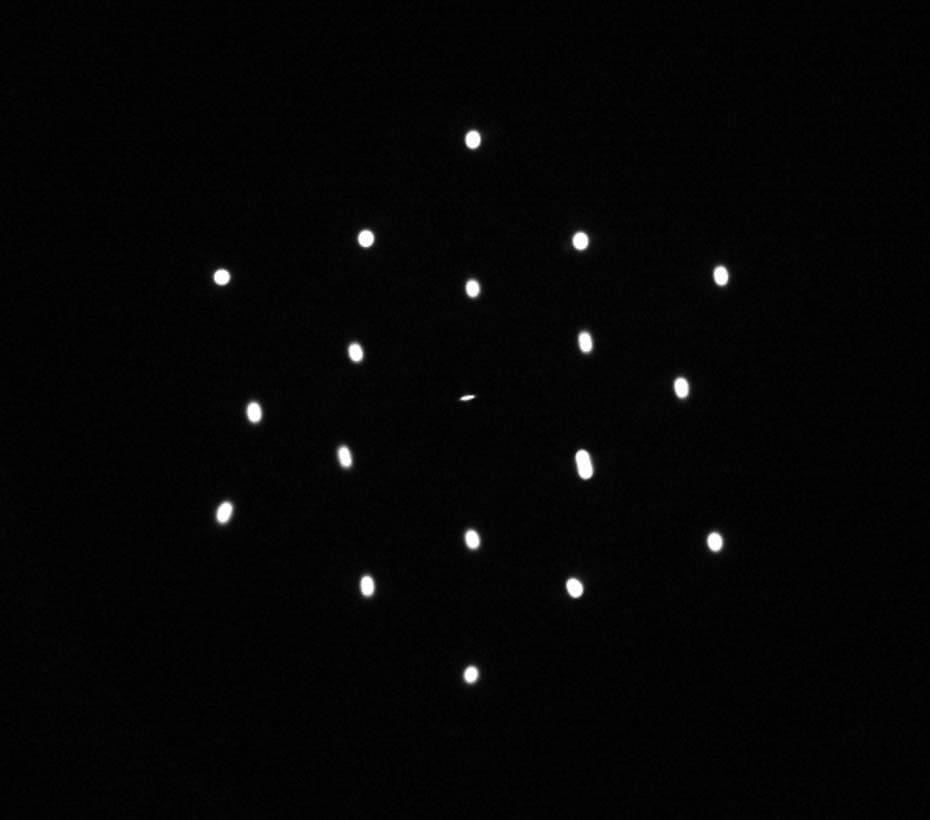
Regarding keratometry, the quality of the measurement is seen in the clarity of the corneal light reflexes (Figure 1). Tear film insufficiencies, corneal dystrophies, and scars will distort the images. Those related to tear film make the reflexes appear smeared (Figure 2) and are improved by instilling an artificial tear and repeating the measurement after 5 minutes.
TROUBLE SHOOTING REQUIRED
We are fortunate to work in a time when our instruments provide feedback for the users regarding the quality of their scans. This, however, does not excuse a technician from understanding what happens during the testing we perform. Our ability to troubleshoot is crucial to providing good patient outcomes. OP

