






When I was just starting as a technologist, I worked for a cornea specialist and a multispecialty general clinic at a busy Level I International Trauma & Burn Center. The job posed a major problem: My retinoscopy was poor so finding a refractive starting point with new patients was difficult.
Yet, using my retinoscopy, a keratometer, and a corneoscope (the only devices I had), one of my strongest skills became my refractions. I learned using keratometry and corneoscope “cheats.” For example, I learned that the steeper the cornea was, the closer the rings were to each other. The axis was identified by where the rings were pulled from a sphere shape to an elliptical shape.
At that time, there were no tomography or topography machines to help with my patients who had cornea trauma, international patients with corneal injuries due to war or environmental issues (vitamin A deficiencies and trachoma), or patients who had corneal eye disease (Fuchs’ endothelial dystrophy, Terrien’s marginal disease, Sjögren's, etc).
You might ask: “If you were working with poor corneas, how could the keratometer be of any use because the images would be difficult, if not impossible, to interpret and use?” And you would be right. Yet the keratometer, which measures only the anterior corneal surface curvature in four locations using Placido rings, was the beginning of the more advanced topography and tomography systems that we use today. (See Table.)
| Manufacturer | Devices | Website |
|---|---|---|
| Alcon | Wavelight Topolyzer Vario | myalcon.com/professional/ |
| Cassini Technologies | Cassini | cassini-technologies.com/ |
| Johnson & Johnson Vision | iDesign | jnjvisionpro.com/products/idesign-refractive-studio |
| Marco/Nidek | OPD-Scan III Wavefront AberrometerOPD-Scan III Visual System | marco.com/product-category/objective-refractors/ |
| Oculus, Inc. | Keratograph 5MKeratograph 4 Easygraph |
us.oculus.de/us/products/topography |
| Pentacam AXL Pentacam HR |
pentacam.com/us/start.html | |
| Tomey | TMS-4N TopographerRT-7000 Multifunctional Auto Ref/K/Topo |
tomeyusa.com/products/cornealtopographers/ |
| Topcon Medical Systems | Aladdin HW 3.0CA-800 Corneal Analyzer | topconhealthcare.com/products/ |
| Tracey Technologies | iTrace | traceytechnologies.com |
| Visionix USA | VX 120+VX 120+ Dry Eye VX 130+ VX 650 |
visionix.com/us/ |
| Carl Zeiss Meditec | Atlas 9000 CornealTopography System | zeiss.com/content/dam/Meditec/us/brochures/atlas.pdf |
| Ziemer Ophthalmics | Galilei G4 ColorZGalilei G6 ColorZ | ziemergroup.com/en/products/diagnostic-devices/ |
A topographer (Figure 1) gives us information of the front surface of the cornea and maps that information.

The tomographer uses the Scheimpflug rotating imaging system that captures scans in a cross-sectional form in a matter of seconds.1 Besides the topographical map, it also provides details regarding anterior and posterior cornea contour, pachymetry, anterior chamber depth, angle evaluation (in glaucoma patients), as well as the pupillary diameter.
This article will present common reasons to perform topography/tomography and discuss testing errors to avoid.
Choosing the right test
There are a number of reasons to perform topography/tomography. Choosing the right test depends on what your doctor is looking for. Some of the issues the provider may try to evaluate are:
- Corneal scarring: changes to the shape of the cornea due to disease or trauma.
- Cornea and/or conjunctival growths: (pterygium, conjunctival tumors, dermoids).
- Contact lens fitting: the fitting/following of gas permeable contact lenses (to ensure the cornea is not being warped or becoming hypoxic [not getting enough oxygen due to a poor fitting lens]).
- Corneal ectasia: when the inner layers of the cornea become weak and cause the cornea to change shape, become thin, and push forward. Keratoconus and pellucid are common reasons for this, but refractive surgery also can cause this issue.2
- High astigmatism: to determine if a patient has keratoconus (coning) versus pellucid (thinning).
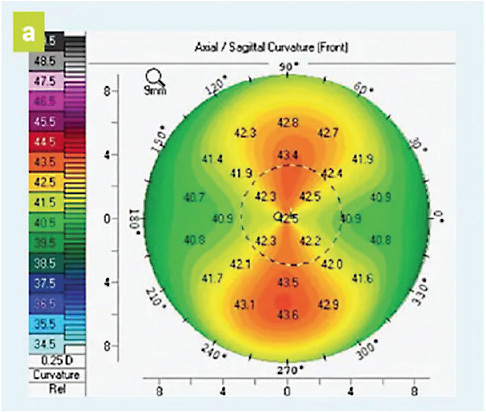
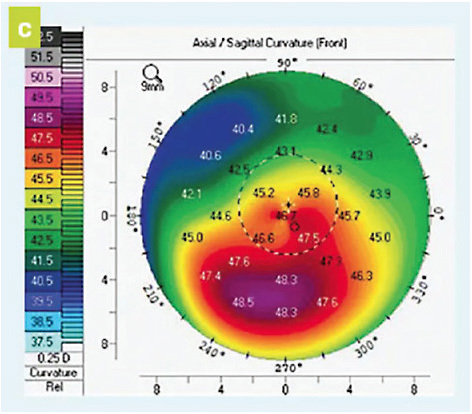
For example: The sagittal maps (Figures 2 and 3) show the color codes that indicate the steepness of the cornea according to its dioptric power. It might be a good indicator that there are higher levels of astigmatism occurring and where the power lies. It is important to rely not only on the color scale but also the dioptric grid shown. In Figure 3, the coning of the cornea is shown as red and orange (warm colors) whereas the flatter area is shown blue and green (cool colors).
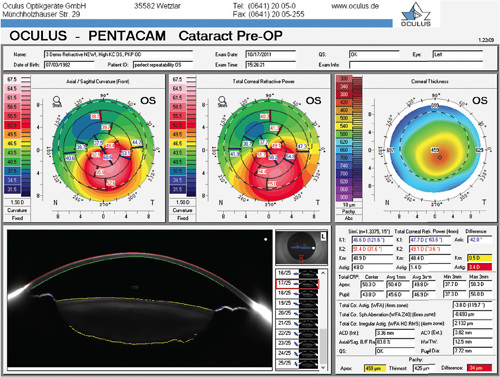
- Refractive surgery. Evaluate pre-/post-refractive status prior to surgery. Figure 4 displays shape and power of the cornea’s anterior and posterior surface and corneal thickness.
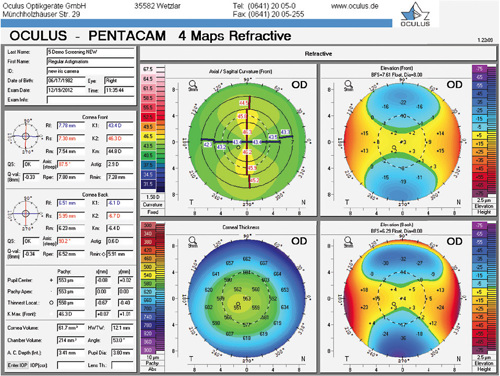
The axial/sagittal map tells us the curvature of the anterior corneal surface in dioptric values for each point. The color scale represents the power in diopters at each particular point. Warmer colors represent steeper corneal curvature, while cooler colors represent flatter areas.
The anterior and posterior elevation maps give us warmer colors where the cornea is elevated above the best fit sphere and cooler colors where the cornea is depressed below the best fit sphere.
The pachymetry map shows corneal thickness. Cooler colors are thicker, and warmer colors are thinner.3
- Cataracts and corneal transplants. Evaluate the cornea prior to cataract surgery to measure: Anterior chamber depth, white to white, pachymetry, keratometry, corneal topography, and appropriate location for limbal relaxing incisions used to decrease post-surgical astigmatism. (Figure 5.)
Types of mapping your doctor may want
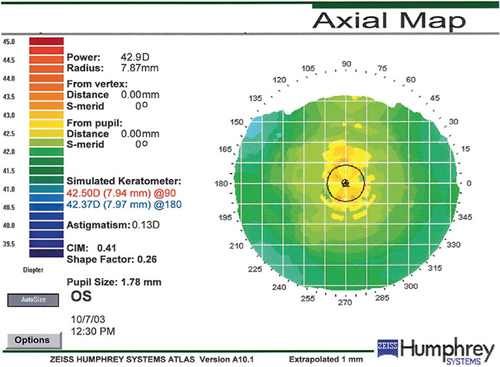
Axial map or sagittal map. As mentioned earlier, the axial map is easy to understand and gives a quick overview average of the curvature of the cornea with a color scale representing the dioptric power at each point (Figure 6). As shown, the warmer colors in the center of the map (red, yellow) represent steeper corneal curvature, while cooler colors (green, blue) represent flatter areas.
Tangential map. It also calculates corneal curvature versus true power but is more sensitive than the axial map. It identifies curvature at individual points versus an average of points. The tangential map is recommended when following advancing keratoconus progression, because it is more sensitive than the generalized axial map. In addition, it is recommended over the axial map when fitting specialty keratoconus contact lenses.
Elevation map. It identifies the difference in the height of the corneal surface when compared to a best-fit spherical surface when fitting gas permeable contact lenses. Shows elevation as well as depressions.
Numerical view. Numerical mapping is useful when fitting specialty contact lenses. It calculates the “average keratometry” value and arranges individual keratometry findings to show curvature readings of the eye.
Tear break-up display map. Tear break-up scores can be measured before starting contact lens wear to evaluate the quality of the tear film and to then see how it is affected by adding a contact lens. Also, the map can be used when taking topography over the top of a contact lens to show the wetting occurring as well as an evaluation of the fit.
Testing errors to be aware of and avoid
- Because the Placido disk mires reflect off the tear, irregularities in the tear film will affect the quality of the Placido disk images. Adding a drop of artificial tears may help with your readings, but do not add a drop that is more viscous than your basic tear, as the added viscous drop can cause false topography mires readings. Remind patients to blink often.
- Show the patient where they are to fixate, and explain what they can expect during the test. This is a quick, non-contact test to perform with the patient’s help. If you don’t explain what to expect, the test can be more difficult than necessary as the patient may look around, may not open their eyes widely, may worry that the machine may touch them, or may ask questions during the test, causing poor positioning.
- Have the patient open their eyes as wide as possible to get the full ring shape, especially superiorly. While taping the lids open is an option to keep the eyelashes from hanging in the image, patients do not like this experience and it can be uncomfortable to remove the tape after the procedure. Hint: Use paper or transpore tape. These are lightweight, gentle on delicate or elderly skin (which can be thinner with aging), and are designed to work even when wet. Be aware: Both stick when the skin is damp, so be gentle when removing from eyelids to prevent skin tearing.
- Learn when contact lens wearers last wore their lenses. Each physician has a recommendation of how long they want a patient to be without contact lens wear prior to testing (some say for RGPs one- to-three months, for soft lenses between one- to-four weeks). Discuss this information at length with the patient when they are scheduled for their appointment. If they arrive and state they did not follow the protocol as requested, they need to be rescheduled.
- Work with your doctor to identify what scan your doctor will want with a given patient. That way, when the patient arrives for the appointment, the tests are done by the technician prior to seeing the doctor and can be discussed at that time versus having to be moved in and out of the exam room.
Using the “tools” available
Looking at all the “tools” you now have available to assist in honing your refractions, your A-scan performance, and your contact lens fitting process—as well as your provider’s ability to detect, assess, and manage any number of corneal diseases—brings to mind the adage, “I wish I knew then what I know now!” There are so many tools that we take for granted. Topography is not just for cornea disease. Using its technology will make your job a lot easier.
Use the “tools” that you have available to improve your general eye exams and the skills you use when performing these technical exams. Instead of them being “just another diagnostic test,” you will appreciate them more for the “hidden cheats” they provide—and your patients will benefit from their advanced exam even more. OP
REFERENCES:
- Scheimpflug Tomography Imaging. Wills Eye Hospital Website. https://www.willseye.org/treatment/scheimpflug-tomography-imaging/ . Accessed April 8, 2023.
- Ectasia Risk in Topography. American Academy of Ophthalmology EyeWiki Website. https://eyewiki.aao.org/Ectasia_Risk_in_Topography . Accessed April 8, 2023.
- Greenwald MF, Scruggs BA, Vislisel JM, Greiner MA. Corneal Imaging: An Introduction. The University of Iowa Ophthalmology and Visual Sciences Website. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Corneal-Imaging/Index.htm . Accessed April 8, 2023.
