







REFRACTOMETRY: THE JACKSON CROSS-CYLINDER REFINES THE REFRACTION
What is the JCC, and why do we use it?
By Sue Corwin, CO, COMT
The Jackson cross-cylinder (JCC) is used to refine both the cylinder axis and cylinder power and give a large change for the patient to give us better responses while keeping the focus on the retina. The lens is composed of two settings: one corresponding to a white dot setting and one corresponding to the red dot setting.
Let’s look at an example of refining cylinder power at 80° with a JCC (see Figure 1).
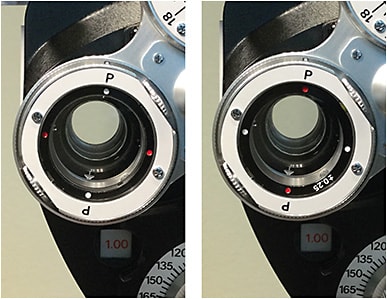
When we place a JCC lens in front of the patient, we do not change the spherical equivalent (SE) — we keep the blur circle on their retina. The formula for SE is sphere + 1/2 cylinder power. So, the white dot setting of -0.25 +0.50 X 80 has an SE of -0.25+0.25 = zero; the red dot setting of +0.25 -0.50 X 80 has an SE of +0.25-0.25 = zero.
We simply ask the patient if they want more cylinder power or less cylinder power, while keeping the focus on the retina. The difference between a +0.50 cylinder power and -0.50 cylinder power is one diopter (D). So, the fact that we keep the focus on the retina and show a large difference (1D) between the two choices makes this lens a powerful tool in refining both cylinder power and axis. This is why our doctors want us to use the JCC, and not ask the question “better one, better two” while changing the cylinder power knob on the refractor.
In our example, the patient has a starting prescription of -3.00 +1.00 x 80 in the refractor. After adjusting the sphere power to get the SE on the retina, we do the cylinder axis refinement then the cylinder power refinement. We have already determined the axis to be 80°. When we “drop down” the JCC in front of the patient’s eye, the -3.00 +1.00 X 80 is already in the refractor, and we add -0.25 +0.50 X 80 to the prescription as the patient looks through the white dot setting. The result is -3.25 +1.50 x 80. Then, we “flip” the JCC to add the red dot setting of +0.25 -0.50 x 80: this result is -2.75 +0.50 X 80. The difference in the white dot cylinder power of +1.50 and the red dot cylinder power of +0.50 is 1D.
In Brief
Luxturna approved by FDA
The FDA has approved Spark Therapeutics’ Luxturna (voretigene neparvovec-rzyl), a one-time gene therapy product indicated for patients with confirmed biallelic RPE65 mutation-associated retinal dystrophy, a rare form of inherited vision loss. This product is the first and only pharmacologic treatment for an inherited retinal disease.
Rhopressa receives FDA approval
Aerie Pharmaceuticals’ Rhopressa (netarsudil ophthalmic solution 0.02%), a once-daily eye drop designed to lower intraocular pressure in patients with open-angle glaucoma or ocular hypertension, received FDA approval. For more, see page 14.
PASCAL Laser to offer PSLT
Topcon Medical Systems’ PASCAL Laser received FDA clearance to offer Pattern Scanning Laser Trabeculoplasty (PSLT) for the reduction of IOP associated with glaucoma. PSLT provides a computer-guided treatment that applies a sequence of patterns onto the trabecular meshwork.
New delivery system for AcrySof IQ
Alcon’s new UltraSert delivery system is pre-loaded with the AcrySof IQ aspheric monofocal IOL. The design allows predictable delivery of the IOL, features a longer 3-mm nozzle tip with a proprietary depth guard, and is for incisions as small as 2.2 mm, the company says.
MINIMALLY INVASIVE GLAUCOMA SURGERY ROUNDUP
MIGS devices and outcomes
January is Glaucoma Awareness Month, an appropriate time to recognize the advances in treatments available to patients who suffer from this disease. (See also “Glaucoma: Novel IOP-lowering drugs” on p. 14.) Among the various treatments available to lower patients’ intraocular pressure (IOP), an emerging trend is toward minimally invasive glaucoma surgery, or MIGS.
Here we present an overview of MIGS devices and procedures, adapted from recent articles in OP and our sister publication, Ophthalmology Management.
iStent
The Glaukos iStent is a 0.3 mm x 1.0 mm stent that is placed within the eye’s natural outflow system, enhancing the eye’s natural, physiological drainage of aqueous humor. In the landmark U.S. Premarket Approval trial that led to FDA approval in 2012, patients with mild to moderate glaucoma were prospectively randomized to cataract surgery alone or combined with an iStent. The visual acuity outcomes, complication rate, and adverse event rate were not measurably significant between the two arms of the study. However, patients receiving the iStent were statistically more likely to be medication-free or take less medication compared to the control arm receiving cataract surgery alone. For more: tinyurl.com/OPMIGS181
Trabectome
The ab interno trabeculectomy, or Trabectome (NeoMedix, Inc.) procedure has been FDA-approved since 2006. This approach employs microincisional technology to enhance the physiological outflow system of the eye. An electrocautery-like device is used to ablate the inner wall of Schlemm’s canal or trabecular meshwork over a portion of the anterior chamber angle, generally 120 degrees. This provides a direct conduit for aqueous humor to leave the eye, again synergistic with the favorable effect of cataract surgery on IOP. For more: tinyurl.com/OPMIGS181
CyPass
The FDA approved Alcon’s CyPass Micro-Stent in June 2016. This device is 6.35-mm long, has a diameter of about 0.5 mm and is implanted with an ab interno approach. It is slightly curved and attached to a guide wire that aids in implantation during gonioscopic visualization. The device tip is used to bluntly dissect the ciliary body from scleral spur and thereby access the suprachoroidal space.
In the COMPASS clinical trial, 374 eyes were randomized to cataract surgery and CyPass implantation, and 131 control eyes were randomized to cataract surgery alone. Unmedicated baseline IOPs were about 24-25 mm Hg. CyPass resulted in an IOP reduction of about 2 mm Hg more than cataract surgery alone at 24 months, and 60% of controls vs. 77% of CyPass subjects achieved ≥ 20% IOP reduction below baseline at 24 months. For more: tinyurl.com/OPMIGS182
XEN
The XEN gel stent offers an alternative — drainage to the subconjunctival space — while using the ab interno approach. Cleared by the FDA in November 2016, the XEN gel stent, is a 6-mm hydrophilic tube composed of porcine gelatin crosslinked with glutaraldehyde. The dehydrated stent is a rigid tube that becomes soft and flexible upon hydration. The XEN offers a 45-micron inner lumen (the 63- and 140-micron lumen XEN are not currently FDA approved). A multicenter, prospective, nonrandomized, open-label international study followed 975 patients undergoing either primary or secondary surgery with either 140-, 63- or 45-micron size lumen for up to 36 months. The mean pre-operative IOP was 22.9 mm Hg on an average of 2.6 medications (no medication washout), and the mean postoperative IOP at 36 months was 13.2 mm Hg on 0.7 medications. For more: tinyurl.com/OPMIGS183
Hydrus
The Hydrus Microstent (Ivantis) is the first intracanalicular stent for Schlemm’s canal. The Hydrus is an 8-mm long, flexible, biocompatible microstent manufactured from nitinol, a nickel titanium alloy that has been used widely in a broad array of implantable medical device technologies. It is delivered via a clear corneal incision and requires the use of a gonioscope. The Hydrus bypasses the trabecular meshwork while also dilating and scaffolding the entire nasal quadrant of Schlemm’s canal. The implantation procedure can be performed in conjunction with cataract surgery or as a standalone surgery.
In the United States, the Hydrus is available for investigational use only. To date, more than 3,300 procedures have been performed worldwide. For more: tinyurl.com/OPMIGS184
GATT
Gonioscopy-assisted transluminal trabeculotomy (GATT) is a novel approach to a circumferential ab interno trabeculotomy in congenital and juvenile glaucoma, adults with various types of open-angle glaucoma (OAG) and in eyes with prior incisional glaucoma surgery. The short- and long-term outcomes of GATT demonstrate that this technique is an effective method for treating various forms of OAG. In a paper presented at the 2015 AAO meeting by Davinder S. Grover, MD, average IOP decreased by 9.2 mm Hg from baseline in a primary OAG group, with a decrease in 1.43 anti-glaucoma medications at 24 months. For more: tinyurl.com/OPMIGS185