A physician advises on staff's role in Preoperative testing for cataract surgery patients
Measurements prior to surgery can have a great impact on visual acuity.
Ophthalmic Professional March 1, 2014Vol 3, Issue March 2014Page(s): 8-11
Surgery
A physician advises on staff’s role in Preoperative testing for cataract surgery patients
Measurements prior to surgery can have a great impact on visual acuity.
Uday Devgan, MD, FACS, FRCS, Los Angeles
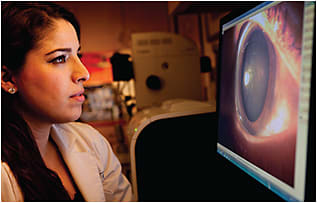
Uday Devgan, MD, and Karen Mrosko, COT, review the corneal topography and higher order optical aberrations in preparation for cataract surgery.
A patient was shocked when I told her that I didn’t need to get an exact refraction prior to her cataract surgery. She wore glasses and contacts for her myopia and astigmatism and had been behind the phoropter dozens of times, comparing lens one to lens two. How could it be that I could give her excellent vision with a cataract surgery and not rely on her refraction?
Cataract surgery is the most commonly performed surgery in the United States and it’s also one of our more powerful refractive tools. At the same time as the cataract surgery, we can correct large degrees of myopia and hyperopia, as well as pre-existing corneal astigmatism. The key concept is that the refraction of the eye measures the refractive state of the whole eye and depends on the cornea, the human lens, and the length of the eye. But with cataract surgery we are removing the human lens, now opaque in nature and called a cataract, and replacing it with a man-made lens implant. And this will have a large impact on the refractive state of the eye.
Routine pre-op testing
In cataract surgery, we are keeping the cornea and axial length of the eye the same, while simply exchanging the cloudy human lens for a clear man-made lens. This means that the two most important measurements before cataract surgery are the corneal power determination via keratometry and the axial length dimension as determined by ultrasound or optical methods.
Sepi Sarshad, COT, reviews anterior segment photos of a cataract patient who is scheduled for upcoming surgery.PHOTOGRAPHY BY MARK HARMEL
While the preoperative refraction is not routinely used to determine the lens power implanted in the eye at the time of cataract surgery, it is still important to measure it accurately. There might be an induced myopia or astigmatism from cataract changes or the opacity may be so much that it severely limits the visual acuity. If a patient has only mild cataract changes and the vision can be corrected to 20/25 with a simple refraction, then perhaps the patient will do well with spectacles alone and surgery could be deferred. Perform a good refraction, but don’t fret if the best-corrected acuity is limited or if the patient has trouble differentiating between similar lens powers.
Corneal biometry
It is important to do corneal measurements before touching the corneal surface like we do for applanation tonometry to measure intraocular pressure. The basic corneal parameter is the determination of the dioptric power using keratometry. This can be done with a manual keratometer or an auto-keratometer, which is often coupled with other devices such as an auto-refractor. For a more advanced look at the cornea, some prefer to do corneal mapping. The two main types of mapping devices are corneal topographers and corneal tomographers, which differ in the way that they image the cornea. The topographers look just at the corneal surface, typically by reflecting concentric rings of light off the tear film. This is why it can be difficult to get readings on patients with dry eyes. The tomographers take many thin-slice section readings of the cornea and then put them together into a composite image. This allows more data, such as the posterior curvature of the cornea and the corneal thickness at any given point. Regardless of the device, the ultimate goal is to determine the power of the cornea and the degree of any pre-existing corneal astigmatism.
Axial length determination
If you’ve ever held a magnifying glass over a newspaper, you know that where you position the lens makes a big difference in focusing the image. When we place an intraocular lens (IOL) implant within the eye during cataract surgery, its final position relative to the retina is key. In eyes that are very myopic, the axial length tends to be longer compared to emmetropic or hyperopic eyes, which are normal and short, respectively.
Sima Tabanfar, OD, measures the intraocular pressure using applanation tonometry.
Above, Karen Mrosko, COT, prepares the corneal topography to measure astigmatism in a cataract surgery patient. At right, After careful biometry with the Zeiss IOL Master (background machine), the higher-order aberrations of the eye are measured using a Nidek OPD scan.
To accurately measure the axial length, we can use an ultrasonic device called an A-scan, which reflects sound waves off the retina and determines the length in millimeters using that data. Optical coherence biometry uses a light beam to accomplish the same measurement, often with a higher degree of precision. Be very careful to take accurate axial length measurements since being off by just one millimeter can make a difference of two to three diopters in the postoperative refractive state of the eye.
IOL calculations
Using the axial length and the power of the cornea, we can use various formulae to calculate the optimal IOL power for cataract surgery. The most commonly used formulae are the Holladay 1, Hoffer Q, and the SRK-T, all of which use simply the keratometry value and axial length data. Newer formulae like the Holladay 2 and Haigis can produce somewhat more accurate results by incorporating other eye dimensions, such as anterior chamber depth and corneal diameter.
The result of the IOL calculations must make sense with respect to the biometry, including the refraction. If you have a patient who has had a similar degree of myopia in both eyes for his entire life and you end up getting different axial lengths and wildly different IOL calculations, a red flag should go up and the measurements repeated. The same way that most people have similarly sized hands or feet, most patients will have similar biometry measurements for each eye.
Concomitant conditions
There are ocular conditions that can affect our preoperative cataract testing and produce less accurate results. On the ocular surface, dry eye syndrome and blepharitis can make corneal measurements challenging. A history of prior corneal refractive surgery such as LASIK can give erroneous keratometry. Even retinal disease such as diabetic retinopathy and macular disease can throw off the axial length measurements.
Cataract surgery coupled with accurate biometry can produce excellent refractive results for our patients, providing a wide range of sharp vision. The cornerstones of our preoperative testing are keratometry to determine the corneal power and axial length biometry. If these are accurate, then the most important refraction that you’ll do is after the cataract surgery, not before. OP
Dr. Devgan is in private practice at Devgan Eye Surgery in Los Angeles, partner at Specialty Surgical Center in Beverly Hills, and Chief of Ophthalmology at Olive View UCLA Medical Center. There are no financial disclosures related to this article. He can be reached at 1-800-337-1969, devgan@gmail.com, www.DevganEye.com.