







Diagnostics
Understanding Visual Field Guided Progression Analysis
How GPA provides clinicians with a tool to differentiate true change from normal variability when evaluating visual fields test results.
Murray Fingeret, OD, New York, NY
Glaucoma is a condition associated with changes in structure to the optic nerve and retinal nerve fiber layer (RNFL). A person’s functional vision is also affected as glaucomatous damage occurs. This damage is evaluated using perimetry (visual fields). While functional loss usually occurs after structural damage has become apparent, both optic nerve evaluation and perimetry are needed in order to establish a diagnosis of glaucoma as well as to monitor the patient over time.
To recognize functional vision loss, an automated perimetry test maps the visual field using a spot of light that is briefly turned on and off at fixed locations. This procedure is performed across the field, usually measuring 54 locations evenly spaced within the central 30 degrees (Figure 1A). Early glaucomatous field defects appear as reduced perimetric sensitivity at several adjacent test points, most commonly in the nasal visual field.
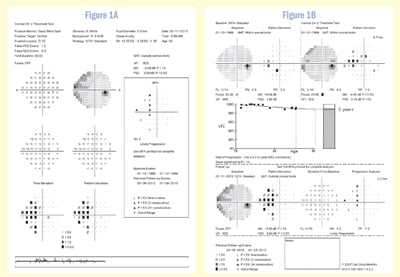
Figure 1A: The results of a perimetry (or visual fields) test. Figure 1B: Guided progression analysis (GPA) produces a “Likely Progression” alert when the same three or more test points are flagged as having changed by statistically significant amounts compared to baseline in three or more tests in a row.
Glaucoma is a chronic condition and may worsen over time. Glaucoma patients are monitored by evaluating the optic nerve, RNFL and visual field for change. If the disease gets worse, areas of visual field loss (scotomas) may increase in size or in severity, or new defects may develop.
Patients Affect Test Results
Visual field testing is a patient task, something the individual must actively participate in, and in that sense it is quite different from retinal photography, which is more of a procedure performed by a technician, with whom the patient merely must cooperate.
Field results are dependent upon patient performance, which may vary test to test. This dependence can lead to defects changing in appearance due to patient performance and not the disease getting worse. Factors that may affect field appearance include patient experience, fatigue and even operator instructions. In regards to experience, it may take up to three tests before a patient is comfortable performing a visual field. As the patient becomes more familiar with performing a perimetric test, each field may appear to be healthier than the one before.
Operator issues are also important, in the sense that patient instruction, coaching and supervision all may be needed to obtain a valid test result. The challenge for the clinician is to determine which fields are truly getting worse, and which ones appear to be changing just because of normal testing variability.
Differentiating Change From Normal Test Variability
The Guided Progression Analysis (GPA, Carl Zeiss Meditec) software program was developed to aid the clinician in differentiating true change from random variability. GPA determines the statistical significance of any observed changes, using a database of glaucomatous individuals who underwent four field tests in a one-month period. Measurement variability increases with advancing damage as well as with increasing distance of the test location from fixation.
The two forms of the GPA, event and trend analysis, complement each other. The event analysis will show which test points have changed by more than amounts expected due to typical testing variability. The trend analysis uses all available data to quantify the rate of change, and thereby helps doctors assess the clinical importance of observed changes.
Event Analysis: Measuring Significant Change
In the event analysis, the first two reliable fields typically are averaged and used as the baseline. Different tests may be chosen as the baseline, for instance, tests completed after significant changes in therapy. Each follow-up field is compared to the baseline, with the pattern deviation test locations analyzed point by point.
If a point has changed by a statistically significant amount one time compared to baseline, an open triangle is seen at that location. If a point changes two tests in a row, a half-filled triangle is seen. When a point changes on three or more consecutive tests, a filled triangle appears (confirmed change). A GPA alert of “Possible Progression” will be found on the bottom of the printout when the same three or more points are flagged two tests in a row. When the same three or more test points are flagged three or more tests in a row, a “Likely Progression” alert is seen (see Figure 1B).
Trend Analysis: Quantifying the Rate of Change
The clinician uses GPA trend analysis to quantify the rate of change for the set of tests and to help determine if the calculated rate of loss may lead to a visual disability. It uses a metric called the Visual Field Index (VFI), which summarizes the entire field as a percentage based upon normal age-corrected sensitivity. VFI is calculated based upon assumed retinal ganglion cell loss with locations weighted differently. For example, central loss is weighted more strongly than peripheral loss in the calculation of VFI. VFI is found on all single field analysis printouts, located just above the global indices on the single field printout. A normal field will have a VFI close to 100% and a perimetrically blind visual field will be at 0%. A VFI approaching approximately 70% is often the point where glaucoma patients first notice something wrong with their vision.
In calculating the trend analysis, each field’s VFI is used as one time point. Five points are needed over at least a two-year time period before the trend analysis can be calculated using a linear regression equation. The trend analysis graph will show the estimated rate of change, with the VFI on the Y axis and the age of the person on the X axis. The GPA summary printout is the most efficient one to use as it shows the baseline fields on top and last field on the bottom, illustrating event analysis.
A trend analysis graph is seen at the bottom of the page (Figure 2A). The GPA printout is available in a two-page format that presents the first two fields and trend analysis on page one (Figure 2A) and the last three fields on page two (Figure 2B).
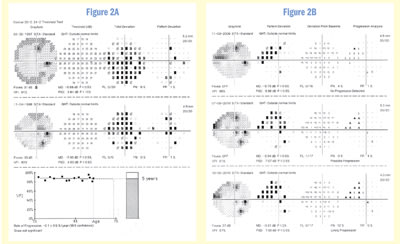
Figure 2A and Figure 2B: The GPA printout is available in a format that presents the two baseline fields and trend analysis on page one (2A) and the most recent three fields on page two (2B).
Tips for Best Test Results
In order to best use the GPA, the same test algorithm, such as SITA Standard, should be used for each test. Also, use the same test pattern with the 24-2 pattern being recommended. The operator may use both 30-2 and 24-2 tests when performing the analysis, but only points common to the 24-2 pattern will be analyzed.
Also when performing perimetry, use the recall patient button if a patient has had fields performed previously. This will ensure the patient’s name and date of birth are always entered consistently, and that each field test result can be included in the analysis. If the name is input differently than on a previous test (e.g., inadvertently adding a letter to the name or changing the birth date) the instrument will recognize the patient as a different patient from the one being evaluated.
Recognizing True Change
An important role for perimetry is to monitor individuals with glaucoma over time to ensure that they are stable and controlled. Fields may change test to test; sometimes due to true change, but other times due to learning, fatigue and random variability. The challenge for the clinician is to recognize which patients really are getting worse and need to have their therapy modified. The GPA program is an important tool that allows the doctor to recognize true change within the visual field. OP

|
Dr. Fingeret is Chief of the Optometry Section, Department of Veterans Administration New York Harbor Health Care System, and Clinical Professor at the State University of New York College of Optometry. He is on the board of directors of the Glaucoma Foundation and past president of the Optometric Glaucoma Society. |